
 “Virginia Democrats believe they have found evidence showing states that expand their Medicaid rolls are better off than those that reject expansion.
“Virginia Democrats believe they have found evidence showing states that expand their Medicaid rolls are better off than those that reject expansion.
…
“Barker said hospitals in states with Medicaid expansion have already benefited from a 30 percent drop in uncompensated care.
…
“The statement is True.”
—PolitiFact Virginia, in an Aug. 10, 2014 fact check of Virginia state senator George Barker (D-Fairfax).
Overview
PolitiFact Virginia performs an incomplete and misleading fact check on uncompensated medical care and the effects of the ACA’s Medicaid expansion.

The Facts
On July 26, 2014 George Barker, a Democratic state senator in Virginia, argued at a political rally that the Affordable Care Act had helped reduce uncompensated care by 30 percent in states that expanded their Medicaid programs under the health care reform law.
A United States Supreme Court decision in 2012 made Medicaid expansion under the ACA optional. About half the states expanded Medicaid, receiving federal funds to help with the increased costs. Other states did not.
PolitiFact Virginia fact-checked Barker’s claim:
“Those states who have adopted Medicaid expansion, and half of the states have — what they have seen just in the first few months of this calendar year, 2014 – is a reduction in uncompensated care,” he said. “That means people who show up at the hospital, show up at the emergency department, are uninsured and can’t pay anything – charity care that’s provided by the hospital – that’s gone down by 30 percent just in the first few months.”
This seems to be an important point for their case, so we wondered about the origin of the figure.
PolitiFact Virginia says the 30 percent figure is correct and gives Barker a “True” rating for his claim.
Analyzing the Rhetoric
We take issue with PolitiFact Virginia’s paraphrasing of Barker, its incomplete research and its implicit-yet-unfounded endorsement of Barker’s underlying argument.
Impaired Paraphrasing
PolitiFact Virginia almost appears to actively try to craft Barker’s words into a defensible statement. When Barker says half the states expanded Medicaid but his supporting data only deal with 15 of them, PolitiFact Virginia covers for the imprecision with the more ambiguous “states” in its paraphrase. When Barker incorrectly defines “uncompensated care” as charity care, PolitiFact Virgina simply omits the mistake from its paraphrase. When Barker says the savings were achieved “just in the first few months,” vaguely implying more savings as more months pass, PolitiFact Virginia again makes the questionable idea disappear from its paraphrase.
PolitiFact Virginia trims away Barker’s rhetorical fat, leaving the relatively lean “Barker said hospitals in states with Medicaid expansion have already benefited from a 30 percent drop in uncompensated care.”
Searching for Research
PolitiFact Virginia locates enough resource material to adequately do its fact check of Barker. But relevant material from PolitiFact Virginia’s list of sources doesn’t find its way into the fact check.
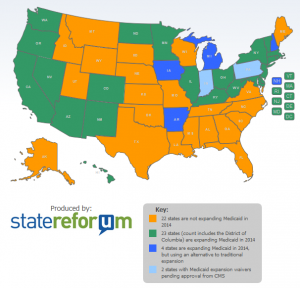
Medicaid expansion map by statereforum.org; click to view offsite
PolitiFact Virginia quotes Barker saying half the states had expanded Medicaid. PolitiFact mentions the Colorado Hospital Association surveyed only 15 of those states in the main study Barker used for support.
PolitiFact Virginia supplemented the evidence from the CHA with reporting from Tenet hospitals and the Arizona Hospital and Healthcare Association, concluding the reduction in uncompensated care looks like a trend.
The fact checker makes no objection to Barker extrapolating the results of these limited studies to apply to all states that expanded Medicaid.
PolitiFact Virginia does something worse than simply draw conclusion about facts on incomplete evidence, however. The fact checkers downplay the part of the story that brings into question Barker’s underlying argument.
Government reimbursement for uncompensated care
The government reimburses some of hospitals’ uncompensated care costs. The Centers for Medicare & Medicaid Services reimburse hospitals through “disproportionate-share hospital payments.” Hospitals bearing a greater burden for uncompensated care receive a larger share of the reimbursement money.
The ACA cuts DSH payments under the expectation that a lower number of uninsured Americans will lead to a decrease in uncompensated care. Barker and PolitiFact Virginia play up the drop in uncompensated care. But if the increase in Medicaid payments doesn’t make up for the loss in DSH payments then who wins? Hospitals may end up worse off with this benefit of the ACA. PolitiFact Virginia recognized this, but did not allow it to lower Barker’s “True” rating (bold emphasis added):
The Governing article said the trend was positive, but hospitals are hoping it’s enough to offset cuts called for in the Affordable Care Act. The biggest piece of this will be $39 billion in cuts to the Disproportionate Share Hospital program, which helps hospitals that serve the poor.
Medicaid underpayment
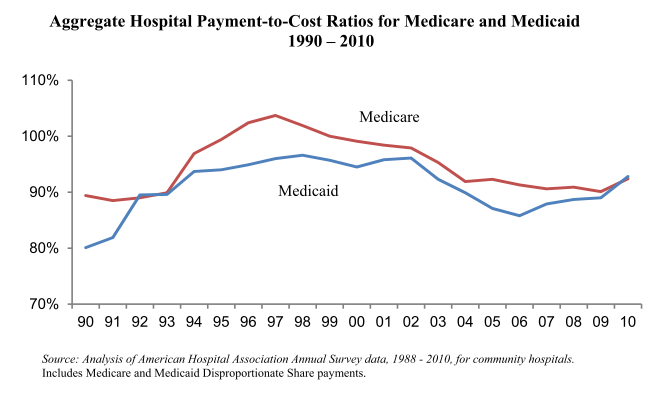
Medicaid and Medicare reimburse hospitals at a rate less than the cost of care. The American Hospital Association explains:
Payment rates for Medicare and Medicaid, with the exception of managed care plans, are set by law rather than through a negotiation process as with private insurers. These payment rates are currently set below the costs of providing care resulting in underpayment.
Hospitals classify these losses separately from uncompensated care. The AHA reported Medicaid reimbursed 89 cents for each dollar of cost for health care services in 2012. If that shortfall remains constant, then an increase in Medicaid patients means a greater financial loss for treating Medicaid patients.
Government may elect to increase reimbursement rates, of course. But hospitals have no guarantee that will occur, especially when cutting reimbursement rates offers government one of its easiest paths toward cutting the budget.
Barker’s Argument
Politicians do not use statistics in speeches for no reason. Barker mentioned the drop in uncompensated care to highlight the success of the ACA. PolitiFact acknowledges this with the first sentence of its fact check—expanding Medicaid makes states “better off”—but only revisits the argument by implying that the accuracy of Barker’s statistic bears out his underlying argument.
In fact, PolitiFact Virginia found information undercutting Barker’s argument. The CHA report, as PolitiFact Virginia noted, said hospitals did not know whether the savings from giving less uncompensated care would make up for the ACA’s other cuts, including cuts to DSH payments.
How does it follow that states expanding Medicaid are better off if the hospitals in those states experience no net gain?
We were able to think of a couple of ways, but PolitiFact Virginia considered neither in its fact check.
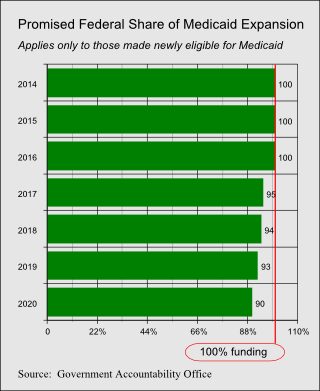
First, if CMS issues DSH reimbursement rules favoring states that expanded Medicaid then those states are arguably better off. However, CMS says its rules do not cut DSH payments as deeply for states refusing to expand Medicaid, perhaps in consideration of the Supreme Court’s ruling that the ACA was unconstitutionally coercive in cutting off federal Medicaid funding to states refusing the ACA’s Medicaid expansion. Still, an evaluation by the Commonwealth Fund predicts citizens in states refusing to expand Medicaid within their own borders will help fund Medicaid in the states accepting the expansion:
Federal funds that pay for state Medicaid programs are raised through federal general revenue collection—taxes paid by residents in all states—whether or not they participate in the program. Therefore, taxpayers in states not participating in the Medicaid expansion will bear a share of the overall cost, without benefitting from the program.
Second, state governments may receive more federal money through ACA-associated programs even if hospitals in those states lose more money treating poor patients. RAND Corporation mathematician Carter C. Price offered this testimony to Congress in 2013:
Our study found that the cost to states for expanding Medicaid generally would be lower than the expense state and local governments will face for providing uncompensated care to uninsured residents after implementation of the Affordable Care Act.
We think Carter’s testimony indulges the ACA’s shell game. Even if the fiscal picture improves for state governments thanks to federal funding, the federal funding comes from the residents of the various states. The Medicaid expansion spends more money, but the federal government taxes the citizens of the states to pay for it instead of making the state governments pay directly. On the other hand, Carter’s point that state governments tend to gain financially by expanding Medicaid is well taken. The federal government taxes states’ citizens and gives the money to the states to spend according to federal guidelines. If the federal government lives up to its promises to fund the Medicaid expansion then the state governments likely come out ahead.
 We think the coercive nature of this relationship makes it controversial whether the states receive a benefit, on balance, by expanding Medicaid. Projected costs are lower for the state governments, but may prove higher for hospitals and the federal government.
We think the coercive nature of this relationship makes it controversial whether the states receive a benefit, on balance, by expanding Medicaid. Projected costs are lower for the state governments, but may prove higher for hospitals and the federal government.
Barker argues that states are better off if hospitals spend about 30 percent less on uncompensated care. If everything else stayed the same, Barker would be right. But the federal government will probably pay more to provide health care for poor people. Hospitals may spend more; studies don’t yet make clear what will happen to the average hospital. State governments may spend less, not counting federal subsidies. But the federal subsidy money ultimately comes from people living in the states.
Given the uncertainties and omitted context, Barker doesn’t have much of an argument. The reduction in uncompensated care provided by hospitals, even if it exceeds 30 percent, gives an unreliable measure of the benefits of the ACA’s Medicaid expansion.
Reviewing PolitiFact Virginia’s Failures
1) PolitiFact Virginia excused, without explanation, a number of inaccuracies in Barker’s statement.
2) PolitiFact Virginia rested its findings on extrapolated data.
3) In the end, PolitiFact Virginia rated Barker on an isolated factoid while ignoring weaknesses it exposed in his underlying argument.
Summary
“evidence showing states that expand their Medicaid rolls are better off than those that reject expansion.”
PolitiFact Virginia frames its fact check as though it is testing Barker’s evidence that state expansions of Medicaid create a benefit for those states. Whether Medicaid expansion makes states better off qualifies as an opinion. More people get insurance through Medicaid, and other people bear the costs. The new arrangement under the ACA represents a complicated set of tradeoffs. We won’t place a truth rating on this matter of opinion. But we note that PolitiFact Virginia’s framing implies cuts to uncompensated care mean states are without question better off with the Medicaid expansion.
“hospitals in states with Medicaid expansion have already benefited from a 30 percent drop in uncompensated care.”
![]()


We find the statement true after stretching to allow a charitable interpretation. The CHA report provides adequate evidence that hospitals in some states saw a 30 percent decrease in uncompensated care. The experience for hospitals in other states may differ. Neither Barker nor PolitiFact Virginia provided information clarifying this point for their audiences. Barker and PolitiFact Virginia presented the savings as a clear benefit even though the CHA report made clear it was uncertain whether the savings from uncompensated care would outweigh the ACA’s cuts to reimbursement. For that omission we charge Barker and PolitiFact Virginia with a fallacy of one-sidedness.
“The statement is True.”
![]()
Barker’s statement was true to the extent we note above, after providing a generously charitable interpretation. However, PolitiFact and its affiliates do not use “true” the same way we do. PolitiFact defines “True” to mean “The statement is accurate and there’s nothing significant missing.” Taken literally, PolitiFact’s definition compels us to rate its claim false. Significant information was left out of the supposedly “True” claim.
The statement is technically true if interpreted charitably, but not “True” as PolitiFact defines it.
References
Madsen, Nancy. “Sen. George Barker Says Uncompensated Care Has Fallen 30 Percent in States That Expanded Medicaid.” PolitiFact Virginia. Tampa Bay Times, 10 Aug. 2014. Web. 17 Aug. 2014.
Rau, Jordan, and Julie Appleby. “Justices Uphold Individual Mandate, Set Limits On Medicaid Expansion.” Kaiser Health News. Henry J. Kaiser Family Foundation, 28 June 2012. Web. 17 Aug. 2014.
“Impact of Medicaid Expansion on Hospital Volumes.” Cha.com. Colorado Hospital Association, June 2014. Web. 18 Aug. 2014.
“States and the Affordable Care Act.” Urban.org. The Urban Institute, n.d. Web. 18 Aug. 2014.
Holahan, John, Linda J. Blumberg, Teresa Coughlin, Brigitte Courtot, Ian Hill, Rebecca Peters, Shanna Rifkin, and Margaret Wilkinson. “The Launch of the Affordable Care Act in Selected States: State Flexibility Is Leading to Very Different Outcomes.” Urban.org. The Urban Institute, Mar. 2014. Web. 18 Aug. 2014.
“Tenet Reports Adjusted EBITDA of $387 Million for the Quarter Ended March 31, 2014.” Tenethealth.com. TH Medical, 05 May 2014. Web. 18 Aug. 2014.
“Search Jobs.” Tenethealth.com. TH Medical, n.d. Web. 18 Aug. 2014.
“Facts about Medicaid Expansion.” Michigan.gov. State of Michigan, n.d. Web. 18 Aug. 2014.
Haynes, Jim. “April 2014 Hospital Financial Results.” Tucson.com. Arizona Hospital and Healthcare Association, 13 June 2014. Web. 18 Aug. 2014.
“From Uncompensated Care to Government Shortfall: Clarifying Key Terms.” Chanet.org. The Center for Health Affairs, Mar. 2013. Web. 18 Aug. 2014.
Kliff, Sarah. “Hospitals Serving the Uninsured Face Challenge under Obamacare.” Washington Post Wonkblog. The Washington Post, 16 Apr. 2013. Web. 18 Aug. 2014.
“Financial Fact Sheets.” Aha.org. American Hospital Association, n.d. Web. 18 Aug. 2014.
“Underpayment by Medicare and Medicaid Fact Sheet.” Aha.org. American Hospital Association, 2014. Web. 18 Aug. 2014.
Angeles, January. “How Health Reform’s Medicaid Expansion Will Impact State Budgets.” Cbpp.org. Center on Budget and Policy Priorities, 25 July 2012. Web. 18 Aug. 2014.
Price, Carter C. “Expanding Medicaid Is the Best Financial Option for States.” RAND.org. RAND Corporation, June 2013. Web. 18 Aug. 2014.
“Medicaid Expansion: States’ Implementation of the Patient Protection and Affordable Care Act.” GAO.gov. United States Government Accountability Office, Aug. 2012. Web. 18 Aug. 2014.
Adair, Bill, and Angie Drobnic Holan. “The Principles of PolitiFact, PunditFact and the Truth-O-Meter.” PolitiFact.com. Tampa Bay Times, 01 Nov. 2013. Web. 18 Aug. 2014.
Related Posts
 Slate helps spread PolitiFact’s false narrative
Slate helps spread PolitiFact’s false narrative PolitiFact stands pat with misleading Bush v. Gore narrative
PolitiFact stands pat with misleading Bush v. Gore narrative More fetal pain follies at LogicallyAI (“Logically Facts”)
More fetal pain follies at LogicallyAI (“Logically Facts”)- Fetal pain follies at LogicallyAI (Updated)
- PolitiFact ‘Mostly’ endorses Kamala Harris falsehood about Florida’s Black history standards (Updated)
 Correction request submitted to Snopes.com, July 16, 2023
Correction request submitted to Snopes.com, July 16, 2023